- Research
- Open access
- Published:
Association between residing in municipalities facing population decline and satisfaction with neighboring healthcare infrastructure in older aged adults
BMC Public Health volume 24, Article number: 2070 (2024)
Abstract
Background
Many municipalities in rural areas of Korea are facing population decline due to the aging population phenomenon. This study examined the relationship between residing in municipalities facing population decline and satisfaction with nearby healthcare infrastructure in older aged adults.
Methods
The 2021 Korea Community Health Survey (KCHS) data were used. Municipalities were classified as those not facing population decline, those at risk, and those facing population decline based on the Population Decline Index. The association between residing in municipalities facing population decline and satisfaction with nearby healthcare infrastructure was examined cross-sectionally using a multi-level logistic regression analysis. Satisfaction with available public transportation was concomitantly examined as it is related to accessing healthcare services.
Results
Of the 58,568 individuals aged 65 years or above analyzed, 27,471 (46.9%) adults were residing in municipalities without population decline, 4,640 (7.9%) adults in municipalities at risk of population decline, and 26,457 (45.2%) in municipalities with population decline. Individuals living in municipalities with population decline were more likely to be dissatisfied with nearby healthcare infrastructure (OR 1.76, 95% CI 1.41–2.20). Similar tendencies were found for public transportation infrastructure (OR 1.67, 95% CI 1.38–2.03).
Conclusions
Individuals residing in municipalities with declining populations are more likely to report dissatisfaction with nearby healthcare infrastructure and public transportation. These findings emphasize the importance of providing adequate medical infrastructure to reduce potential health-related disparities.
Introduction
South Korea is one of the most rapidly aging countries in the world and is projected to become a super-aged society, wherein 20% of its population is aged 65 years or older, by 2026 [1]. This phenomenon is the result of the country’s low birth rate, which has continued for nearly two decades and has led to natural population decline (Supplementary Fig. 1) [2]. As the population dwindles, many rural municipalities are at risk of extinction and may soon disappear [3]. This tendency has been influenced by population aging and strong youth migration, wherein many younger individuals are migrating to the capital city, Seoul, and its nearby areas to seek higher-quality tertiary education and jobs [4]. In fact, the population of the capital region accounts for a large proportion of the entire Korean population [5]. Population aging and concentration in the capital area have left many rural local municipalities at risk of extinction, generally characterized by having a high proportion of older adults.
Rural communities are characterized by lower availability of healthcare resources and personnel [6]. Additionally, as rural municipalities are largely composed of older adults who have a greater need for healthcare and medical services, they are likely to face greater difficulties in adequately accessing healthcare services [7]. A prerequisite for the adequate delivery of healthcare services is the availability of suitable healthcare infrastructure, including buildings, beds, and equipment [8, 9]. Although healthcare infrastructure is important for delivering and improving healthcare quality, there are often large regional discrepancies in its distribution owing the limited availability of resources [9]. Considering that health infrastructure is cited as critical infrastructure in many countries, which generally refers to facilities and services that are essential for the basic functioning and well-being of a society, [10] there is a need to explore the adequacy of healthcare infrastructure in rural municipalities facing rapid population decline.
Another characteristic of many local municipalities is that they are situated in rural municipalities with comparatively poor public transportation, which can act as a barrier to accessing healthcare services in a timely manner, leading to negative health outcomes [11]. Specifically, inadequate transportation can result in lost or delayed appointments, poorer compliance, and reduced routine healthcare visits in older adults [11,12,13]. As such hindrances to public transportation can lead to poorer health outcomes and higher disease burden, accounting for access to public transportation alongside healthcare services is important [11].
The objective of this study was to investigate whether residing in municipalities facing population decline is associated with lower levels of satisfaction with nearby healthcare infrastructure in older aged adults. Healthcare infrastructure was analyzed alongside public transportation as it is an important factor in accessing medical services. The hypothesis was that residents of local municipalities characterized by population decline would report lower levels of satisfaction with nearby healthcare infrastructure and public transportation.
Methods
Data and study population
This study used data from the 2021 Korea Community Health Survey (KCHS), a cross-sectional survey conducted annually by the Korea Disease Control and Prevention Agency (KDCA). The KDCA uses the computer-assisted personal interview method to perform in-person interviews with a sample representative of the Korean population. The study population was selected from national census data using a stratified, multistage, probability cluster sampling method [14]. The KCHS data consisted of 229,242 individuals, in which 74,492 individuals were aged 65 years or above. Of the 74,492 individuals, those with missing values on the outcome variable or the variables were excluded from the study population. The final study population included 58,568 individuals (Fig. 1).
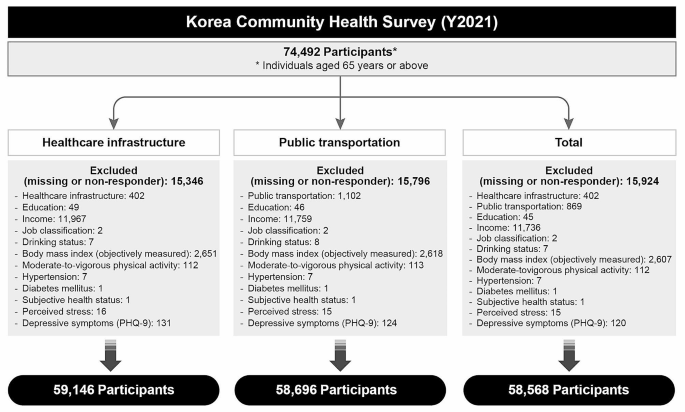
Flow-chart of study participants selection process
Outcome measure
The outcome measure was satisfaction with the healthcare infrastructure and public transportation available nearby in the municipalities in which the participants resided. This was measured using the following questions: “Are you satisfied with the healthcare infrastructure (community health center, clinics and hospitals, and pharmacies) available in your residing neighborhood?” “Are you satisfied with the available public transportation (bus, taxi, subway, or train)? respectively.” Participants responded to these questions with either “yes” or “no.”
Independent variables
The main independent variable was the population decline status of 255 municipalities in Korea, which was measured using the Population Decline Index. The “Special Act on Balanced National Development” was introduced by the government in 2016 to cope with the issue of population decline in rural municipalities. Based on this Act, the Ministry of Public Administration and Security reports on municipalities facing population decline, which is measured based on the summation of changes in the average annual population growth rate, population density, net youth (individuals aged 19–34) mobility rate, daytime population size, aging (individuals aged 65 or above) rate, youth proportion (individuals aged < 14) rate, crude birth rate, and financial independence of the municipality (Supplementary Table 1). The 2021 report classified 89 municipalities with population decline and 18 municipalities at risk of population decline (Fig. 2). This study categorized municipalities into three groups based on this index: “municipalities without population decline,” “municipalities at risk of population decline,” and “municipalities with population decline.” The Population Decline Index was successfully evaluated in a previous study [15].

Municipalities categorized according to the Population Decline Index
Various covariates were considered in this analysis. The included variables were sex (male or female), age (65–69, 70–74, 75–79 or 80 + years), educational level (none, elementary school, middle school, high school, or college or above), income (quartiles), job classification (professional or administrative position, office work, sales and service, agriculture and fishery, blue collar work or simple labor, or unemployed), smoking status (no or yes), monthly drinking (no or yes), Body Mass Index (BMI; underweight, normal, or obese), moderate to vigorous levels of physical exercise (no or yes), hypertension (no or yes), diabetes (no or yes), subjective health status (poor or fair), perceived stress (no or yes), and depressive symptoms (no or yes). A BMI of < 18.5 was categorized as underweight, 18.5≤, < 25.0 as normal, and ≥ 25.0 as obese [16]. Depressive symptoms were defined based on the Patient Health Questionnaire-9, which ranges from 0 to 27 with a cutoff score of 10 [17].
Statistical analysis
The chi-square test was used to examine the general characteristics of the study population. The association between satisfaction with nearby infrastructure and residing in municipalities facing population decline was analyzed using a multilevel logistic regression analysis. The null hypothesis was examined in Model 1, individual-level factors in Model 2, and both individual- and municipal-level factors in Model 3. A random intercept model with municipality as a level 2 variable was used in the full fitting model. The latent variable method of intra-cluster correlation (ICC), Median Odds Ratio (MOR), and proportional change in variance were used to reveal the variation measures that infer random effects. Specifically, the MOR is a useful measure to interpret the magnitude of the contextual effect [18, 19]. The goodness of fit was compared between models using the − 2 log likelihood test, Akaike Information Criteria (AIC), and Bayesian Information Criteria (BIC). From this, Model 3 was shown as the best fitting model. Results are presented as Odds Ratios (OR) and 95% Confidence Intervals (CI). Statistical significance was set at p < 0.05. All analyses were conducted using SAS software (version 9.4, SAS Institute, Cary, NC, USA).
Ethical approval
The Korea Community Health Survey (KCHS) data are openly published. Participant’s data were fully anonymized prior to release. Our study was excluded from the review list pursuant to Article 2.2 of the Enforcement Rule of Bioethics and Safety Act in Korea, since the data was exempted from IRB review. All procedures performed in studies involving human participants were in accordance with the ethical standards of the national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Results
The general characteristics of the study population are presented in Tables 1 and 2. In total, 27,471 (46.9%) individuals resided in municipalities without any risk of population decline, 4,640 (7.9%) resided in municipalities at risk of population decline, and 26,457 (45.2%) resided in municipalities with population decline. A higher percentage of individuals residing in at-risk municipalities (21.9%) or municipalities with population decline (24.5%) reported dissatisfaction with the healthcare infrastructure available nearby compared to those residing in municipalities with no risk of population decline (16.6%). Similar trends were observed for public transportation. Overall, the socioeconomic status of participants residing in areas with population decline were lower. The results of the descriptive statistics on health status according to the Population Decline Index can be found in Supplementary Table 2.
Information of the random effects in the model and model fit is presented in Table 3. The null model (Model 1) confirmed the fitness of the multilevel analysis in which ICC was calculated to show the intra-cluster variability of the study population. The results of Model 1 also showed that the intraclass correlation coefficient ranged from 14.7–18.6%, which indicates that 14.7–18.6% of the variation in satisfaction with nearby healthcare infrastructure and public transportation can be attributed to differences between clusters. The MOR indicates that when individuals with identical characteristics are randomly selected from different clusters, the participant from the higher-risk cluster has 2.05–2.29 times higher odds of being satisfied with nearby healthcare infrastructure and public transportation. As Model 3 (the fully adjusted model) of the three models analyzed in this study had the lowest AIC and BIC scores, this model can be seen as the best fitting model
The results of the multilevel analysis of the association between municipalities with population decline and the likelihood of dissatisfaction with nearby infrastructure are presented in Fig. 3. Individuals residing in municipalities with population decline were more likely to be dissatisfied with nearby healthcare infrastructure (OR 1.76, 95% CI 1.41–2.20). Similar tendencies were found for public transportation infrastructure (OR 1.67, 95% CI 1.38–2.03). The results on other types of infrastructure, namely safety-related infrastructure (natural disasters, traffic accidents, agricultural accidents, and crime), environmental conditions (air and water quality), and living conditions (electricity, sewage system, waste system, and sport facilities) are presented in Supplementary Table 3 for reference.

Results of the multilevel analysis on the association between residing in regions with population decline and dissatisfaction with nearby healthcare infrastructure and public transportation. The adjusted odds ratios were adjusted for sex, age, education, income, job, smoking, drinking, body mass index, moderate-to-vigorous physical activity, hypertension, diabetes, subjective health status, perceived stress, and depressive symptoms
Discussion
This study investigated whether individuals residing in municipalities with population decline report higher levels of dissatisfaction with nearby healthcare infrastructure and public transportation. The results revealed that individuals residing in municipalities with population decline, particularly those in municipalities facing extinction, are more likely to report dissatisfaction with the nearby healthcare infrastructure. Similar tendencies were reported for public transportation
Considering that the majority of municipalities facing population decline or extinction are located in non-urban areas, the findings of this study are generally in accordance with previous literature that reported a deficiency in infrastructure for the provision of medical services in rural regions [20]. Regional disparities have been reported in Korea as healthcare personnel and medical equipment tend to be concentrated in urban regions, with over half of the major medical resources, including personnel and infrastructure, located in the capital area [21]. Unsurprisingly, access to medical services is poor in rural, mountainous, and seaside areas [22]. Similar tendencies have been found in other countries, where inadequate access to medical services is documented in rural areas [23]. Such disparities may be of particular significance in municipalities with an aging population because individuals residing in rural municipalities report an excessively greater burden of age-related health conditions and frailty than urban dwellers [24, 25]. Limited access to medical services and resources has been cited as a major barrier to alleviating disparities in age-related health conditions in rural populations. The results suggest the need to monitor and implement health policies that can moderate regional disparities in healthcare [24].
Beyond healthcare infrastructure, individuals residing in municipalities characterized by population decline report difficulties in accessing public transportation, which is important because it is inevitably linked to access to medical services. Transportation has been cited as the most influential element in achieving healthcare accessibility, with a significant association between means of transportation and medical use [26, 27]. Specifically, because rural dwellers need to travel longer distances to access healthcare, inadequate transportation can exacerbate disparities as it can result in lost appointments or delayed healthcare, which in turn can result in poorer health outcomes and a greater disease burden [11, 28]. A relationship has been found between transportation convenience and unmet healthcare needs in older adults living in rural areas [29]. Studies have shown that the unavailability of mobile vehicles or door-to-door transportation mechanisms can lead to higher barriers in accessing and utilizing medical services in older adults [12, 30]. Unsurprisingly, older adults without access to adequate transportation services have been found to be more likely to forego or delay healthcare appointments for care [31, 32]. These findings suggest the importance of reducing transportation-related barriers to improve healthcare accessibility and mitigate health-related regional disparities.
This study has some limitations. First, the possibility of residual confounding factors could not be completely ruled out, although the analysis was adjusted for various covariates. For instance, certain characteristics possibly related to the level of satisfaction with nearby healthcare infrastructure and public transportation, such as car ownership, could not be accounted for as they were not measured in the data used. Second, the analysis could not consider online medical services, which is related to accessibility to health care services, due to data limitations. Reimbursement of telehealth services for medical consultation and medicine prescription is currently being operated as a pilot program. Last, information on the health status, such as diabetes, of the participants were measured based on self-reports in the KCHS. As such, this study did not analyze the potential effect of health status on the association between residing in municipalities facing population decline and satisfaction with neighboring healthcare infrastructure. Future studies incorporating the limitations state above are needed. Despite the limitations stated above, this study is unique in that it is the first to investigate whether residing in municipalities facing population decline is associated with lower levels of satisfaction with nearby healthcare infrastructure and public transportation. The study results are particularly noteworthy because many rural municipalities in Korea currently face population decline due to population aging, when there is a need to provide adequate healthcare infrastructure in rural municipalities.
Conclusions
Individuals residing in municipalities with population decline, particularly those in municipalities facing extinction, are more likely to report dissatisfaction with nearby healthcare infrastructure and public transportation. Considering the large number of municipalities expected to experience population decline due to aging, most of which are located in rural municipalities, these findings emphasize the importance of providing adequate medical infrastructure in these municipalities to reduce potential health-related disparities.
Data availability
Data will be made available on request. The dataset is available on the Korea Community Health Survey website (http://chs.kdca.go.kr/chs/rdr/rdrInfoPledgeMain.do).
References
Kim KW, Kim OS. Super Aging in South Korea Unstoppable but Mitigatable: a sub-national Scale Population Projection for best policy planning. Spat Demogr. 2020;8(2):155–73.
Cho KA. Korea’s low birth rate issue and policy directions. Korean J Women Health Nurs. 2021;27(1):6–9.
Chung S. The risk of local extinction in South Gyeongsang Province. Korean Reg Sociol. 2019;20(2):87–104.
Lee S-L, Youth Migration. Population Concentration in the Capital Region, and Population Crisis in non-capital regions. Res Brief Korea Inst Health Social Affairs. 2021;72:1–8.
Chun Y, Kim K. Temporal changes in the urban system in South Korea. Front Sustain Cities. 2022;4:1013465.
Gizaw Z, Astale T, Kassie G. What improves access to primary healthcare services in rural communities? A systematic review. BMC Prim Care. 2022;23:313.
Nielsen M, D’Agostino D, Gregory P. Addressing Rural Health challenges Head on. Mo Med. 2017;114(5):363–6.
Scholz S, Ngoli B, Flessa S. Rapid assessment of infrastructure of primary health care facilities - a relevant instrument for health care systems management. BMC Health Serv Res. 2015;15:183.
Lan T, Chen T, Hu Y, Yang Y, Pan J. Governmental Investments in Hospital infrastructure among regions and its efficiency in China: an Assessment of Building Construction. Front Public Health. 2021;9:719839.
Gallais C, Filiol E. Critical infrastructure: where do we stand today? A comprehensive and comparative study of the definitions of a critical infrastructure. J Inform Warfare. 2017;16(1):64–87.
Bove AM, Gough ST, Hausmann LRM. Providing no-cost transport to patients in an underserved area: impact on access to physical therapy. Physiother Theory Pract. 2019;35(7):645–50.
Syed ST, Gerber BS, Sharp LK. Traveling towards disease: transportation barriers to health care access. J Community Health. 2013;38(5):976–93.
Okoro C, Strine T, Young S, Balluz L, Mokdad A. Access to health care among older adults and receipt of preventive services. Results from the behavioral risk factor surveillance system, 2002. Prev Med. 2005;40:337–43.
Kang YW, Ko YS, Kim YJ, Sung KM, Kim HJ, Choi HY, et al. Osong Public Health Res Perspect. 2015;6(3):211–7. Korea Community Health Survey Data Profiles.
Ju YJ, Kim W, Chang K, Lee TH, Lee SY. Patients with diabetes in regions with population decline and likelihood of receiving diabetes management education and screenings for related complications in Korea. Prev Med 2023:107793.
Weir CB, Jan A. BMI classification percentile and cut off points. In: StatPearls. Treasure Island (FL); 2023.
Levis B, Benedetti A, Thombs BD, Collaboration DESD. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:l1476.
Merlo J, Chaix B, Ohlsson H, Beckman A, Johnell K, Hjerpe P, et al. A brief conceptual tutorial of multilevel analysis in social epidemiology: using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J Epidemiol Community Health. 2006;60(4):290–7.
Larsen K, Merlo J. Appropriate assessment of neighborhood effects on individual health: integrating random and fixed effects in multilevel logistic regression. Am J Epidemiol. 2005;161(1):81–8.
Lee J. Urban-rural differences in intention to age in place while receiving home care services: findings from the National Survey of older koreans. Arch Gerontol Geriatr. 2022;101:104690.
Eun SJ. Trends and disparities in avoidable, treatable, and preventable mortalities in South Korea, 2001–2020: comparison of capital and non-capital areas. Epidemiol Health. 2022;44:e2022067.
Lee S. Spatial and socioeconomic inequalities in accessibility to Healthcare Services in South Korea. Healthc (Basel) 2022;10(10).
Coombs N, Campbell D, Caringi J. A qualitative study of rural healthcare providers’ views of social, cultural, and programmatic barriers to healthcare access. BMC Health Serv Res. 2022;22:438.
Jang IY, Jung HW, Lee CK, Lee YS, Kim KI, Kim KW, et al. Rural and Urban Disparities in Frailty and Aging-Related Health conditions in Korea. J Am Geriatr Soc. 2016;64(4):908–11.
Yu P, Song X, Shi J, Mitnitski A, Tang Z, Fang X, et al. Frailty and survival of older Chinese adults in urban and rural areas: results from the Beijing Longitudinal Study of Aging. Arch Gerontol Geriatr. 2012;54(1):3–8.
Arcury TA, Preisser JS, Gesler WM, Powers JM. Access to transportation and health care utilization in a rural region. J Rural Health. 2005;21(1):31–8.
Rosenthal TC, Fox C. Access to health care for the rural elderly. JAMA. 2000;284(16):2034–6.
Ricci-Cabello I, Ruiz-Perez I, Rojas-Garcia A, Pastor G, Goncalves DC. Improving diabetes care in rural areas: a systematic review and meta-analysis of quality improvement interventions in OECD countries. PLoS ONE. 2013;8(12):e84464.
Choi Y, Nam K, Kim C-Y. Association between Convenience of Transportation and Unmet Healthcare needs of Rural Elderly in Korea. J Prev Med Public Health. 2019;52(6):355–65.
Kullanit A, Taneepanichskul N. Transportation barriers on Healthcare utilization among Elderly Population living in Mahasarakham Province, Thailand. J Health Res. 2017;31:233–8.
Fenton JJ, Von Korff M, Lin EH, Ciechanowski P, Young BA. Quality of preventive care for diabetes: effects of visit frequency and competing demands. Ann Fam Med. 2006;4(1):32–9.
Mattson J. Transportation, Distance, and Health Care utilization for older adults in rural and small urban areas. Transp Res Rec. 2011;2265:192–9.
Acknowledgements
The authors would like to thank Woohyun Cho (Medical Information & Media Center, Ajou University School of Medicine) for helping with the figure included in this paper.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (Ministry of Science and ICT) (No. NRF-2022R1C1C2003977). The funding source had no involvement in the study design, data analysis and interpretation, writing of the manuscript or in the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
YJJ, WK, and SYL contributed to the concept of the study. YJJ and SYL contributed to the acquisition and analysis of data. WK, KC, and THL drafted the work. All authors revised the final draft and approved the submitted version of the manuscript.
Corresponding author
Ethics declarations
Ethical approval
This study used the Korea Community Health Survey data, which are open data that contain no personal information. All personal information was anonymized prior to release. The data used were exempt from IRB review in accordance with the review list pursuant to Article 2.2 of the Enforcement Rule of Bioethics and Safety Act in Korea. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
One of the authors, Yeong Jun Ju, is an editorial board member of BMC Public Health. All the other authors declared no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ju, Y.J., Kim, W., Chang, K. et al. Association between residing in municipalities facing population decline and satisfaction with neighboring healthcare infrastructure in older aged adults. BMC Public Health 24, 2070 (2024). https://doi.org/10.1186/s12889-024-19410-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19410-z