- Research
- Open access
- Published:
The effect of psychological interventions targeting overweight and obesity in school-aged children: a systematic review and meta-analysis
BMC Public Health volume 23, Article number: 1478 (2023)
Abstract
Background
Multi-component psychological interventions may mitigate overweight and obesity in children and adolescents. Evidence is, however, scattered on the effectiveness of such interventions. This study aims to review the available evidence on the effectiveness of multi-component psychological interventions on anthropometric measures of school-aged children with overweight or obesity.
Methods
We systematically searched international databases/search engines including PubMed and NLM Gateway (for MEDLINE), Web of Science, SCOPUS, and Google Scholar up to November 2022 for relevant articles pertaining to psychological weight-loss interventions targeting school-aged children. Two reviewers screened and extracted pertinent data. The quality of included studies was assessed using the Cochrane Risk of Bias Tool for Randomized Trials. Random effect meta-analysis was used to calculate, and pool standardized mean differences (SMD). We distinguished between intervention and maintenance effects. Intervention effects were defined as the mean change in outcome measurement detected between baseline and post-treatment. Maintenance effects were defined as the mean change in outcome measurement between post-treatment and last follow-up.
Results
Of 3,196 studies initially identified, 54 and 30 studies were included in the qualitative and quantitative syntheses, respectively. Most studies reported on group-based interventions. The significant effects of intervention on BMI z-score (SMD -0.66, 95% CI: -1.15, -0.17) and WC (SMD -0.53, 95% CI: -1.03, -0.04) were observed for interventions that centered on motivational interviewing and cognitive behavioral therapy, respectively. Mean BMI and WC did not differ significantly between post-treatment and last follow-up measurement (maintenance effect), indicating that an initial weight loss obtained through the intervention period could be maintained over time.
Conclusions
Findings indicate that motivational interviewing and cognitive behavioral therapy as interventions to reduce BMI z-score (generalized obesity) and waist circumference (abdominal obesity) are effective and durable. However, detailed analyses on individual components of the interventions are recommended in future effectiveness studies.
Background
The global burden of non-communicable diseases (NCDs) has increased over recent years [1, 2]. NCDs accounted for 7.1 million additional deaths in 2019 compared to 2009 globally [3]. Obesity is a prominent risk factor for many NCDs, including cardiovascular diseases, type 2 diabetes, cancer, disability, and death [1,2,3]. Over two thirds of the key drivers of NCDs (e.g., unhealthy diet, physical inactivity, obesity) are formed or emerge during childhood and adolescence [4]. Therefore, prevention must start with this age group at both national and global levels.
Recent estimates based on 2416 data sources showed that between 1975 and 2016, the global prevalence of obesity increased from 0.7 to 5.6% in girls and from 0.9 to 7.8% among boys aged 5–19 years [5]. There is also evidence showing a positive association between childhood obesity and the development of NCD risk factors in adulthood [2]. This underscores the urgent need to address overweight and obesity already in childhood.
Several studies indicate that diet therapy, exercise, and education, along with parent education, may be effective approaches to reduce obesity among children and adolescents [6,7,8,9]. There is also evidence suggesting that combining behavioral (e.g., diet or physical activity interventions) and psychological methods (e.g., cognitive behavioral therapy or motivational interviewing) in multi-component interventions might enhance weight reduction among children with obesity above and beyond single-component interventions [10, 11]. In addition, this evidence indicates that maintenance of weight loss over time might be more difficult to achieve than the initial weight reduction. So, the main goal of psychological interventions in obesity management is to provide effective interventions to make changes that are durable [10, 11]. However, existing evidence on the efficacy of these types of multi-component interventions in terms of weight-loss maintenance is somewhat scattered—especially related to child populations [10]. To our knowledge there are currently no published systematic reviews or meta-analyses that have addressed effectiveness of psychological intervention on obesity management. Therefore, this study aims to review the existing evidence on the efficacy of child weight-loss interventions that include a psychological intervention component.
The present study addresses the following research questions: 1) What kind of psychological interventions have been applied so far targeting overweight and obesity in school-aged children? 2) What are the most effective psychological intervention methods for reducing overweight and obesity among school-aged children? 3) What are the strengths and limitations of each of the intervention designs and/or methods in terms of efficacy, durability, and implementation?
Definition of psychological interventions
In the broadest terms, psychological interventions relate to non-pharmacological interventions that target cognitive, behavioral, emotional, interpersonal, social, or environmental factors to improve a particular health outcome or condition [12]. They involve psychological therapies (e.g., cognitive behavioral therapy), education and social support approaches, social environment and norm-based strategies, or a combination of these [12].
Psychological therapy in overweight and obesity may include, for example, cognitive behavioral therapy (CBT), motivational interviewing (MI), or acceptance therapy [13]. Psychological interventions may be individual, or group based [12]. For maximum effect, these interventions usually are applied in the context of a multi-component weight loss program (e.g., dietary and exercise strategies as a behavioural therapy) [13].
Methods
Identification of relevant studies
We conducted the present study according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guideline (PRISMA) (Fig. 1) [14]. The study protocol has been published in the International Prospective Register of Systematic Reviews (PROSPERO), registration number: CRD42022309438.

Flow diagram of study selection
The search strategy was developed to target three key focus areas: Psychological interventions, overweight/obesity, and school-aged children (See Additional file 1 for the full search strategy). The search included studies published up to and including November 2022. No language or geographical limitation were applied. The optimal sensitivity of searching for articles, was reached by simultaneous search of the most comprehensive databases/ search engines including PubMed and NLM Gateway (for MEDLINE), Web of Science (ISI/WOS), SCOPUS, and Google Scholar. Further, reference lists of the included publications or reviews were studied to identify potentially eligible studies that were missed in the database searches. Relevant book chapters were also reviewed for data. If multiple publications were based on a single study, just one publication was included. Duplicates and non-peer reviewed publications were excluded.
Primary outcomes
Change in anthropometric measures (weight, body mass index (BMI), BMI z-score, waist circumference (WC), waist-to-height ratio (WhtR), percentage overweight) represented the primary outcome.
Secondary outcomes
Changes in body composition, blood pressure, biomarkers of metabolic-syndrome, behavioral measures (e.g., dietary intake, physical activity), and measures of quality of life (e.g., perceived physical and mental health) were secondary outcomes.
Inclusion and exclusion criteria
The inclusion criteria are as follow
1- The study population was limited to school-aged children (6–18 years old). 2- Participants in each study had overweight or obesity according to any parameter (e.g., BMI, BMI z-score, WC, WhtR, percent body fat). 3- Studies comprised randomized controlled trials (RCTs) or quasi-randomized controlled trials (QRCTs) which had applied any kind of psychological interventions for weight loss in school-aged children with overweight or obesity.
The exclusion criteria are as follow
1- Studies without a primary outcome of obesity reduction 2- Observational studies/ non-randomized controlled trials 3- Studies on participants with prevalent disease, eating disorder (e.g., anorexia nervosa) or special needs besides overweight interventions 4- Studies that had combined pharmacological intervention on obesity with psychological interventions 5- Studies without sufficient information to determine eligibility.
Quality assessment
Two researchers conducted the systematic literature review, study-quality assessment, and the data extraction. Any inter-rater discrepancies were resolved by a third party. The extracted data included author and year of publication, country, population characteristics (e.g., age), and methodology (e.g., study design, sample size, type of psychological intervention/theory, duration of intervention, and outcomes.
The quality assessment for each of the included studies was done using the Cochrane Risk of Bias tool (RoB2) for randomized controlled trials [15]. The RoB2 comprises five domains of potential bias. These include bias in the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in outcome measurement, and bias in the reporting of results [15]. Employing the validated RoB2 algorithm (available at https://methods.cochrane.org/bias/), each domain was assessed in terms of three levels of risk of bias: low risk, some concerns, or high risk.
Data extraction
Outcome data were extracted from baseline, post-treatment, and subsequent follow-up measurement. Intervention effects were defined as the mean difference in outcome measurement detected between baseline and post-treatment in both control and intervention groups. Maintenance (effectiveness) was defined as mean difference in outcome between the post-treatment and last follow up measurement. If multiple follow-up data were provided, the last follow-up data were used for estimation of maintenance effect size.
Statistical analysis
Heterogeneity among studies was assessed using the chi-square-based Q-test and the I-squared statistic. A random-effects meta-analysis model using the Hedges method [16] was used when heterogeneity was statistically significant (Q-test < 0.1).
Standardized mean differences (SMDs) and 95% confidence intervals (CIs) were used to determine intervention effect sizes in terms of the primary and secondary outcomes.
Subgroup analysis was performed with respect to intervention duration (≤ 6 month, > 6 month), age category (≤ 12-year-old, > 12-year-old), intervention design (group-based, individual-based), intensity of the intervention (low, moderate, high), and type of control group (active, passive, routine care, and no-intervention).
Hours of contact was calculated as a proxy for intensity of the interventions. The figures were categorized as very low (< 10 h), low (10–25 h), moderate (26–75 h), or high (> 75 h) [17].
Control group type was determined based on the study information.
Publication bias was assessed with Egger's test at a significance level of p < 0.1.
A meta-regression analysis was conducted to find the sources of heterogeneity. All analyses were conducted using Stata 17 (version 17; Stata Corp, College Station, Texas).
A limited number of studies included secondary outcomes (e.g., quality of life, dietary outcomes). Of these studies, heterogeneity across studies in terms of methodology, outcome measurement, and type of intervention precluded an accurate meta-analysis of these outcomes. For this reason, our findings that relate to secondary outcomes are presented only but qualitatively.
Results
Findings from systematic review
Study selection process
A total of 3,196 studies was identified in the initial database search. An additional three articles were identified through citation searching. After deduplication, 3,014 articles remained. A total of 2,874 articles was excluded based on screening titles and abstracts. Of the remaining 140 studies, 86 were excluded after the full-text review. The most common reasons for exclusion related to study design (non-RCT), the intervention lacking psychological components and/or not targeting a relevant outcome, or not providing sufficient information about the studied population (Fig. 1). Ultimately, 54 studies were eligible for inclusion in the systematic review [7, 18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70].
Study characteristics
The characteristics of the included studies on the efficacy of psychological interventions targeting overweight and obesity in school-aged children are demonstrated in Additional file 2. Most of the studies (41 out of 54 included studies) were published within the recent 10 years (as of 2023), indicating increasing focus on this topic as a global public health challenge.
Most studies (n = 31) were conducted in the US [18, 20, 22,23,24, 28, 30, 32, 34, 36,37,38, 40, 41, 43, 45,46,47,48,49, 51, 54, 55, 60, 61, 65, 66, 68,69,70], followed by Iran [19, 29, 57, 62], UK [33, 53, 63], Denmark [31, 35], the Netherlands [42, 58], China [39, 67], Israel [27, 52], Germany [7], Spain [21], Iceland [25], Turkey [26], Norway [44], Belgium [50], Switzerland [64], Australia [56], and Mexico [59].
Sample sizes ranged from 27 participants in a call-based intervention [32] to 549 in a community and clinic-based intervention [39]. Cognitive therapy alone or in combination with other behavioral methods was the most applied approach in the included studies [18,19,20,21,22, 27,28,29,30, 34, 36, 37, 42, 44, 48, 50, 55, 56, 58, 61, 64, 65, 68]. BMI z-score and BMI were the most frequently used outcome measures [18, 20, 21, 23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59, 61,62,63,64,65,66,67,68,69,70].
All studies applied multi-component psychological interventions based on either nutritional and/or physical activity programs for weight reduction. Quality of life (QL) [18, 19, 47, 54, 60, 63], dietary intakes [18,19,20, 23, 29, 39, 45, 48, 66], and physical activity (PA) [19,20,21, 23, 34, 39, 48, 63] were measured using a wide range of assessment tools.
Intervention duration ranged from 1.5 months in a day-camp and home setting intervention [31] to 36 months [20] (intervention setting was not provided by the researchers). Intervention sessions were variable (e.g., daily, or monthly basis). Follow-up time ranged from 2.5 months [31] to 24 months [27, 35]. In more than half of the studies (35/54), intervention groups were compared with control groups, while in the rest of the studies two or three intervention groups were compared. The reported interventions were implemented by people from a wide range of academic and professional backgrounds (e.g., school nurse, psychologist) and educational levels (e.g., master-level instructors, professional intervention delivery agent). Overall, most studies used professionals to implement the interventions, whereas in one study [51], intervention was delivered by using, an automated interactive voice response system (machine).
Type of psychological interventions
As illustrated in Additional file 2, different types of psychological interventions were applied and evaluated in the reviewed studies (e.g., cognitive behavioral, motivational interviewing).
Psychological intervention designs
Figure 2 summarizes different psychological intervention designs used in the included studies. Group-based interventions represented the most common intervention design. Most interventions targeted both children and their parents [18,19,20,21, 24,25,26,27, 30, 32, 35,36,37,38,39, 41, 43, 46, 48, 50, 51, 55, 57,58,59, 61, 62, 64, 66,67,68,69,70]. Individual designs were applied in five studies that focused on children or adolescents [23, 28, 33, 34, 54].
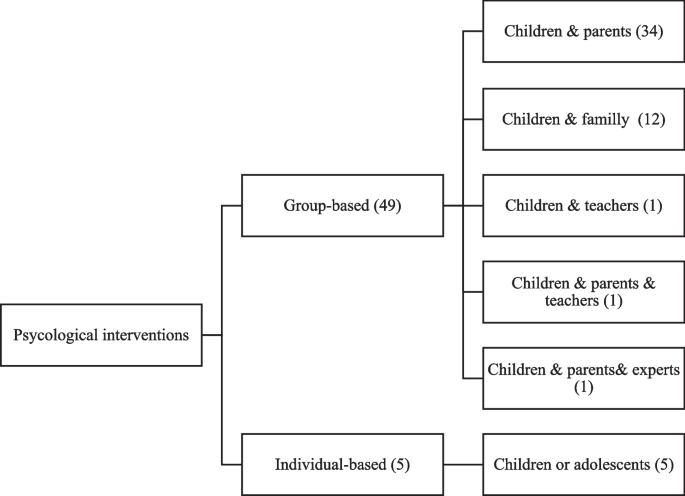
Psychological interventions designs targeting overweight, and obesity in school-aged children (based on studies included in systematic review)
Strengths and limitations of the intervention designs and methods
Table 1 illustrates strengths and limitations of different psychological designs adapted from [21, 58, 71,72,73,74,75,76,77,78,79,80,81,82] additionally with authors’ opinion. Furthermore, the following paragraph provide an overview on the main strengths and limitations of the most prominent psychological intervention methods- adapted from [83,84,85], additionally with authors’ opinion.
As the most frequent method in the reviewed studies, CBT covers a wide range of psychological aspects and social consequences of obesity from anxiety and loneliness to weight loss. It can also facilitate long-term weight-maintenance skills and improve a person’s self-esteem and -image. However, it also has limitation meaning that CBT alone will not work for everyone with obesity. So, it might be combined with other interventions like lifestyle changes to provide better results on obesity management.
MI alone, or in combination with CBT, also featured in the reviewed studies. MI has a strong theoretical foundation that emphasizes the importance for the individual to recognize and internalize why change is necessary and how change can be achieved. However, this highly individualized approach is also a limitation as implementation requires extensive tailoring to the target individual or group.
Findings from meta-analysis
Of the 54 included studies, 30 were eligible for inclusion in the meta-analysis [7, 18,19,20, 23, 24, 27,28,29,30, 33, 34, 36, 37, 39, 40, 44, 48, 50,51,52,53,54, 57,58,59,60,61, 65, 67]. Reasons for excluding 24 studies from further analysis were due to several issues (e.g., having unclear, insufficient, or missing data). The combined sample size of RCT studies included in the meta-analysis totaled 4093 school-aged children with overweight or obesity.
The pooled intervention effect is shown in Table 2. The intervention effect was statistically significant on all BMI measures (BMI and BMI z-score) (SMD: -0.59, 95% CI: -0.89, -0.20, I2 = 96.64), BMI z-score (SMD: -0.39, 95% CI: -0.69, -0.09, I2 = 88.60) and BMI (SMD: -0.79, 95% CI: -1.48, -0.09, I2 = 97.80). We also detected statistically significant intervention effects on fat mass (SMD: -0.96, 95% CI: -1.54, -0.38, I2 = 85.00), body fat (SMD: -0.81, 95% CI: -1.30, -0.33, I2 = 69.29), and diastolic blood pressure (SMD: -0.49, 95% CI: -0.83, -0.15, I2 = 41.80).
The pooled maintenance effect of intervention is shown in Table 3. Mean BMI and WC did not differ significantly between post-treatment and last follow-up measurement, indicating that initially lost weight is not regained during a subsequent follow-up period (maintenance effect).
Table 4 shows the results of sub-groups meta-analyses by type, duration, design, and intensity of psychological intervention, population age, and type of control group. In sub-group analyses the significant effect of psychological interventions on BMI was observed in studies conducted on children > 12 years old (SMD = -0.79, 95% CI: -1.57, -0.01), group-based interventions (SMD = -0.98, 95% CI: -1.80, -0.16), intervention of moderate intensity (SMD = -1.40, 95% CI: -2.56, -0.23), and interventions with a passive control group (SMD = -0.41, 95% CI: -0.79, -0.02). Moreover, the significant effect of psychological interventions on BMI z-score was observed in studies with very low (SMD = -0.88, 95% CI: -1.20, -0.56) or moderate intervention intensity (SMD = -0.96, 95% CI: -1.83, -0.10), or studies conducted with treatment-as-usual control group (SMD = -0.86, 95% CI: -1.04, -0.67). Significant effects on WC were observed in studies with low intervention intensity (SMD = -0.34, 95% CI: -0.59, -0.09) or studies conducted with passive control groups (SMD = -0.24, 95% CI: -0.44, -0.04).
MI and CBT—as effective psychological interventions—significantly reduced BMI z-score (generalized obesity) (SMD = -0.66, 95% CI: -1.15, -0.17) and WC (abdominal obesity) (SMD -0.53, 95% CI: -1.03, -0.04), respectively.
The highest pooled SMD in BMI z-score (SMD -0.96, 95% CI: -1.83, -0.10) was observed in interventions of moderate intensity.
Figure 3 shows forest plot of intervention effects on BMI measures in our target population.

Forest plot of psychological intervention effect on BMI measures in school-aged children with overweight and obesity
Meta-regression
Sufficient data were available to perform a meta-regression analysis of intervention effect on BMI z-score, BMI, and WC by intervention type, duration, design, and intensity, age, and type of control group. Meta-regression of BMI-z score showed that age (coefficient: -0.77, SE: 0.22; p < 0.100), intervention intensity (coefficient: 0.18, SE: 0.08; p < 0.100), and type of control group (coefficient: -0.42, SE: 0.14; p < 0.100) contributed to the heterogeneity. No sources of heterogeneity were found for BMI and WC.
Quality of the studies
The kappa statistic for agreement of quality assessment was 0.90. The quality assessment of the included studies is presented in Additional file 2. Of 54 included studies, 22 (41%) were rated as low risk of bias. While eight studies were rated as high risk of bias. For the rest of the studies there were some concerns about the risk of bias.
Publication bias
The result of Egger’s test revealed no substantial risk of publication bias neither for the intervention effect outcomes, nor for the maintenance ones (p-value > 0.1).
Discussion
Our study revealed that several different types of psychological interventions targeting school-aged children with overweight, or obesity have been trialed. CBT alone or in combination with other behavioral methods was the most frequently applied approach in the reviewed studies.
Selection of an appropriate psychological approach for successful weight management plan depends on creating a good connection with educational interventions [86]. So, researchers, professional health care providers, and general practitioners (GPs) who are working with overweight or obesity of school-aged children are encouraged to consider such conjunctions for an effective weight management plan.
Our findings also revealed that group-based interventions which rely on parents to implement lifestyle strategies were the most common method for managing overweight and obesity in the reviewed studies. This may depend on that parents’ engagement can support and facilitate the process of obesity treatment that requires a combination of strategies for lifestyle and behavioral changes [87]. We also believe that parents are very important for success in any kind of the interventions for weight management by helping children to commit to new healthy lifestyle activities. On the other hand, parents have some level of control over their children’s dietary and lifestyle environments such that they might be able to prevent health-risk behaviors and facilitate health-promoting behaviors. Therefore, researchers are more willing to engage parents on obesity management interventions.
In our study strengths and limitations of each psychological intervention designs and methods was presented. We think that the design-based research is an appropriate approach to creating feasible and more effective intervention programs that address overweight and obesity- as complex health problems. By understanding such details (strengths and limitations), researchers and professionals will be able to strengthen intervention implementation, evaluation, and sustainability. Besides, this part of our study will support researchers for identification of potential challenges as well. However, we think that there are differences between methodological ideals that we have presented here and the real-life intervention context. So, such differences should be determined in future studies. For example, proper implementation of CBT requires engaging trained employees and target groups who are willing to receive this type of therapy to achieve the maximum benefit for obesity management. Therefore, CBT may not generally be a cost-effective method for the health care system as well as the society in the long term. However, we know that weight loss is a complex problem that involves issues (e.g., body image, self-image, confidence, etc.,) so that CBT can be a useful psychological intervention in several stages of the weight management program. So, we argue that researchers or health authorities should make the final and case-specific decisions regarding implementation of this type of intervention based on their resources including human, financial resources, and time, etc. They should also think if the advantages outweigh the disadvantages for the target population as well as the healthcare system in the long run. MI as another psychological method respects the patient's autonomy and it will work properly for losing weight. Nevertheless, it requires trained staff in weight loss programs. So, we believe it might not be generally supported by the health sector especially primary health care providers. GPs with previous therapeutic training might be interested to apply such methods in weight management plans, though this should be tested in real-life interventions. Alternatively, staff specifically trained in these methods should be used.
In the present meta-analysis, we combined non-family interventions (e.g., children and teachers) with family-based interventions into a general group-based intervention format. The rationale for such a combination was the limited number of studies which had applied non-family intervention design. This might have affected the results of our study. Mainly because family dynamics (e.g., communication pattern, interaction between family members, etc.) as well as culture, family norms, parents’ beliefs and health perception might influence the effectiveness of weight management programs, while such influence might not be seen in non-family groups. For instance, parents who perceive their child’s overweight or obesity as a genetic inheritance might not feel the need to modify their unhealthy lifestyle [88], because they do not consider excess-weight or even obesity as a modifiable risk factor for overall health of their children. We believe that adverse effects of family characteristics on the efficacy of the interventions might affect even well-defined treatment plans. So, for the design and implementation of future theory-based treatment interventions, researchers, GPs, and other health authorities are encouraged to be more focused on family elements (e.g., family norms, parents’ health perception) associated with healthy behaviors. Eventually we argue that future interventions should be socially and culturally adapted for the target population to gain more success and sustainability in obesity management plan, however effectiveness of such approach should be trialed.
In our meta-analysis, we also evaluated effectiveness of 30 studies that included psychological interventions for obesity management. In a previous study, researchers could not make a firm conclusion about the effectiveness of psychological interventions for childhood obesity [10]. But our findings demonstrated benefits of psychological interventions specifically CBT and MI for obesity management. Therefore, our findings both fill the above-mentioned knowledge gap and specify the direction of future research which will be discussed in the following.
In terms of intervention components, our findings revealed that interventions with “moderate-intensity” are more effective than the other types of intervention intensity for reducing BMI and BMI z-score (generalized obesity). Meaning that, these kinds of interventions produced the largest reduction in BMI and BMI z-score among the studied population. However, WC (abdominal obesity) improved significantly with “low intensity” interventions. A previous study showed short-term benefits of comprehensive medium- to high-intensity behavioral interventions in children and adolescents with obesity [17]. The presently discussed interventions appear to offer effects that are durable for the follow-up period subsequent to the intervention. However, we argue that the combination of cognitive and motivational techniques with behavioral therapies with more focus on intervention components should be trialed in future studies because it will probably improve the maintenance of positive effects on obesity management.
Strengths and limitations of the study
This is the first comprehensive study to investigate the effectiveness of multicomponent psychological interventions on managing overweight and obesity among school-aged children. However, the current study also has limitations. First, we excluded some of the studies from the meta-analysis due to a variety of reasons (e.g., lack of sufficient data on primary outcomes of obesity, not having a control group). So, due to sample size limitation we were unable to perform subgroup analyses for all obesity outcomes and this may affect our conclusion on the effect of the interventions. Second, the combination of non-family interventions with family-based interventions- as “group-based” interventions might also affect the results of our study as family and non-family-based groups might be unequal. Family groups are more likely to have a connection and some sort of shared identity than non-family groups have, which may dilute the overall effect of group-based interventions if these two group formats are combined and treated as one. Therefore, this important limitation should also be considered in future studies.
Conclusion
Evaluated interventions showed benefits of CBT and MI as psychological interventions targeting school-aged children with overweight and obesity. Hence, such kind of interventions for weight management of our target population is recommended. It is also important that existing psychological interventions in conjunction with other treatment methods are tested and continually improved for more sustainability in obesity management as well as improvements on other health outcomes and quality of life. Furthermore, authors would like to suggest conducting more studies to explore and apply family characteristics, social elements or other factors affecting efficacy and adherence of the interventional programs. Finally, we suggest that differences between methodological ideals and the real-life intervention context should be determined in future studies by asking for feedback from GPs, professional healthcare providers, and patients who are engaged in the intervention implementation.
Availability of data and materials
The original contributions presented in the study are included in the article as supplementary material. Further inquiries can be directed to the corresponding authors.
Abbreviations
- NCDs:
-
Non-Communicable diseases
- CBT:
-
Cognitive behavioral therapy
- MI:
-
Motivational interviewing
- PRISMA-P:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis guideline
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- ISI/WOS:
-
Web of Science
- BMI:
-
Body mass index
- WC:
-
Waist circumference
- WhtR:
-
Waist-to-height ratio
- RCTs:
-
Randomized controlled trials
- QRCTs:
-
Quasi-randomized controlled trials
- RoB2 :
-
Cochrane Risk of Bias tool
- QL:
-
Quality of life
- PA:
-
Physical activity
- SMD:
-
Standardized mean differences
- CI:
-
Confidence interval
- SE:
-
Standard error
- GPs:
-
General practitioners
- HC:
-
Hip Circumferences
- BP:
-
Blood Pressure
- LDL:
-
Low Density Lipoprotein
- HDL:
-
High Density Lipoprotein
- TG:
-
Triglycerides
- TC:
-
Total Cholesterol
- WHR:
-
Waist to Hip Ratio
- NP:
-
Not Provided
References
Kim J, Lee I, Lim S. Overweight or obesity in children aged 0 to 6 and the risk of adult metabolic syndrome: a systematic review and meta-analysis. J Clin Nurs. 2017;26(23–24):3869–80. https://doi.org/10.1111/jocn.13802. Epub 2017 May 23. PMID: 28295797.
Karnik S, Kanekar A. Childhood obesity: a global public health crisis. Int J Prev Med. 2012;3(1):1–7 PMID: 22506094; PMCID: PMC3278864.
GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–88. https://doi.org/10.1016/S0140-6736(18)32203-7. Epub 2018 Nov 8. Erratum in: Lancet. 2019 Jun 22;393(10190):e44. Erratum in: Lancet. 2018 Nov 17;392(10160):2170. PMID: 30496103; PMCID: PMC6227606.
Guariguata L, Jeyaseelan S. Children and Non-communicable disease, Global Burden Report, 2019.
Biswas T, Townsend N, Huda MM, Maravilla J, Begum T, Pervin S, Ghosh A, Mahumud RA, Islam S, Anwar N, Rifhat R, Munir K, Gupta RD, Renzaho AMN, Khusun H, Wiradnyani LAA, Radel T, Baxter J, Rawal LB, McIntyre D, Mørkrid K, Mamun A. Prevalence of multiple non-communicable diseases risk factors among adolescents in 140 countries: A population-based study. EClinicalMedicine. 2022;52:101591. https://doi.org/10.1016/j.eclinm.2022.101591.
Saelens BE, Grow HM, Stark LJ, Seeley RJ, Roehrig H. Efficacy of increasing physical activity to reduce children’s visceral fat: a pilot randomized controlled trial. Int J Pediatr Obes. 2011;6(2):102–12. https://doi.org/10.3109/17477166.2010.482157. Epub 2010 Jun 7. PMID: 20528109; PMCID: PMC3010313.
Reinehr T, Schaefer A, Winkel K, Finne E, Toschke AM, Kolip P. An effective lifestyle intervention in overweight children: findings from a randomized controlled trial on “Obeldicks light. Clin Nutr. 2010;29:331–6. https://doi.org/10.1016/j.clnu.2009.12.010. Epub 2010 Jan 27. PMID: 20106567.
Bae JH, Lee H. The effect of diet, exercise, and lifestyle intervention on childhood obesity: a network meta-analysis. Clin Nutr. 2021;40(5):3062–72. https://doi.org/10.1016/j.clnu.2020.11.006. Epub 2020 Nov 11. PMID: 33223118.
Mead E, Brown T, Rees K, Azevedo LB, Whittaker V, Jones D, Olajide J, Mainardi GM, Corpeleijn E, O’Malley C, Beardsmore E, Al-Khudairy L, Baur L, Metzendorf MI, Demaio A, Ells LJ. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst Rev. 2017;6(6):CD012651. https://doi.org/10.1002/14651858.CD012651. PMID: 28639319; PMCID: PMC6481885.
Bogle V, Sykes C. Psychological interventions in the treatment of childhood obesity: what we know and need to find out. J Health Psychol. 2011;16(7):997–1014. https://doi.org/10.1177/1359105310397626. Epub 2011 Mar 28. PMID: 21444728.
Rankin J, Matthews L, Cobley S, Han A, Sanders R, Wiltshire HD, Baker JS. Psychological consequences of childhood obesity: psychiatric comorbidity and prevention. Adolesc Health Med Ther. 2016;7:125–46. https://doi.org/10.2147/AHMT.S101631. PMID: 27881930; PMCID: PMC5115694.
Haslam C, Jetten J, Cruwys T, Dingle GA, Haslam SA. The new psychology of health unlocking the social cure. Routledge; 2018.
Vallis TM, Macklin D, Russell-Mayhew S. Canadian Adult Obesity Clinical Practice Guidelines: Effective Psychological and Behavioural Interventions in Obesity Management. Available from: https://obesitycanada.ca/guidelines/behavioural. Accessed [date].
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–41. https://doi.org/10.1016/j.ijsu.2010.02.007. Epub 2010 Feb 18. Erratum in: Int J Surg. 2010;8(8):658. PMID: 20171303.
Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, Cochrane Bias Methods Group; Cochrane Statistical Methods Group. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. https://doi.org/10.1136/bmj.d5928.
Hedges LV, Olkin I. Statistical methods for meta-analysis. Academic press; 2014.
Whitlock EP, O’Connor EA, Williams SB, Beil TL, Lutz KW. Effectiveness of weight management interventions in children: a targeted systematic review for the USPSTF. Pediatrics. 2010;125(2):e396–418 Epub 2010 Jan 18. PMID: 20083531.
Janicke DM, Lim CS, Perri MG, Mathews AE, Bobroff LB, Gurka MJ, Parish A, Brumback BA, Dumont-Driscoll M, Silverstein JH. Featured article: behavior interventions addressing obesity in rural settings: the E-FLIP for kids trial. J Pediatr Psychol. 2019;44(8):889–901. https://doi.org/10.1093/jpepsy/jsz029. PMID: 31039250; PMCID: PMC6705715.
Miri SF, Javadi M, Lin CY, Griffiths MD, Björk M, Pakpour AH. Effectiveness of cognitive-behavioral therapy on nutrition improvement and weight of overweight and obese adolescents: a randomized controlled trial. Diabetes Metab Syndr. 2019;13(3):2190–7. https://doi.org/10.1016/j.dsx.2019.05.010. Epub 2019 May 22. PMID: 31235156.
Moore SM, Borawski EA, Love TE, Jones S, Casey T, McAleer S, Thomas C, Adegbite-Adeniyi C, Uli NK, Hardin HK, Trapl ES, Plow M, Stevens J, Truesdale KP, Pratt CA, Long M, Nevar A. Two family interventions to reduce BMI in low-income urban youth: a randomized trial. Pediatrics. 2019;143(6):e20182185. https://doi.org/10.1542/peds.2018-2185. PMID: 31126971; PMCID: PMC6565337.
Sepúlveda AR, Solano S, Blanco M, Lacruz T, Veiga O. Feasibility, acceptability, and effectiveness of a multidisciplinary intervention in childhood obesity from primary care: Nutrition, physical activity, emotional regulation, and family. Eur Eat Disord Rev. 2020;28(2):184–98. https://doi.org/10.1002/erv.2702. Epub 2019 Dec 4. PMID: 31802570.
Wilson TA, Liu Y, Adolph AL, Sacher PM, Barlow SE, Pont S, Sharma S, Byrd-Williams C, Hoelscher DM, Butte NF. Behavior modification of diet and parent feeding practices in a community- vs primary care-centered intervention for childhood obesity. J Nutr Educ Behav. 2019;51(2):150–161.e1. https://doi.org/10.1016/j.jneb.2018.05.010. Epub 2018 Aug 20. PMID: 30139562.
Bean MK, Ingersoll KS, Powell P, Stern M, Evans RK, Wickham EP 3rd, Mazzeo SE. Impact of motivational interviewing on outcomes of an adolescent obesity treatment: results from the MI values randomized controlled pilot trial. Clin Obes. 2018;8(5):323–6. https://doi.org/10.1111/cob.12257. Epub 2018 Jun 21. PMID: 29931804; PMCID: PMC6158038.
Crespo NC, Talavera GA, Campbell NR, Shadron LM, Behar AI, Slymen D, Ayala GX, Wilfley D, Elder JP. A randomized controlled trial to prevent obesity among Latino paediatric patients. Pediatr Obes. 2018;13(11):697–704. https://doi.org/10.1111/ijpo.12466. Epub 2018 Sep 26. PMID: 30257069; PMCID: PMC6420225.
Njardvik U, Gunnarsdottir T, Olafsdottir AS, Craighead LW, Boles RE, Bjarnason R. Incorporating appetite awareness training within family-based behavioral treatment of pediatric obesity: a randomized controlled pilot study. J Pediatr Psychol. 2018;43(9):1017–27. https://doi.org/10.1093/jpepsy/jsy055. PMID: 30010923.
Sen M, Uzuner A, Akman M, Bahadir AT, Borekci NO, Viggiano E. Examination of a board game approach to children’s involvement in family-based weight management vs. Traditional family-based behavioral counseling in primary care. Eur J Pediatr. 2018;177(8):1231–8. https://doi.org/10.1007/s00431-018-3177-z. Epub 2018 May 29. PMID: 29845514.
Yackobovitch-Gavan M, Wolf Linhard D, Nagelberg N, Poraz I, Shalitin S, Phillip M, Meyerovitch J. Intervention for childhood obesity based on parents only or parents and child compared with follow-up alone. Pediatr Obes. 2018;13(11):647–55. https://doi.org/10.1111/ijpo.12263. Epub 2018 Jan 17. PMID: 29345113.
Annesi JJ, Walsh SM, Greenwood BL, Mareno N, Unruh-Rewkowski JL. Effects of the Youth Fit 4 Life physical activity/nutrition protocol on body mass index, fitness and targeted social cognitive theory variables in 9- to 12-year-olds during after-school care. J Paediatr Child Health. 2017;53(4):365–73. https://doi.org/10.1111/jpc.13447. Epub 2017 Jan 4. PMID: 28052570.
Bagherniya M, Sharma M, Mostafavi Darani F, Maracy MR, Safarian M, AllipourBirgani R, Bitarafan V, Keshavarz SA. School-based nutrition education intervention using social cognitive theory for overweight and obese Iranian adolescent girls: a cluster randomized controlled trial. Int Q Community Health Educ. 2017;38(1):37–45. https://doi.org/10.1177/0272684X17749566. Epub 2018 Jan 3. PMID: 29298634.
Wilfley DE, Saelens BE, Stein RI, Best JR, Kolko RP, Schechtman KB, Wallendorf M, Welch RR, Perri MG, Epstein LH. Dose, content, and mediators of family-based treatment for childhood obesity: a multisite randomized clinical trial. JAMA Pediatr. 2017;171(12):1151–9. https://doi.org/10.1001/jamapediatrics.2017.2960. PMID: 29084318; PMCID: PMC6169780.
Larsen KT, Huang T, Ried-Larsen M, Andersen LB, Heidemann M, Møller NC. A multi-component day-camp weight-loss program is effective in reducing BMI in children after one year: a randomized controlled trial. PLoS One. 2016;11(6):e0157182. https://doi.org/10.1371/journal.pone.0157182. PMID: 27362497; PMCID: PMC4928840.
Daly P, Pace T, Berg J, Menon U, Szalacha LA. A mindful eating intervention: a theory-guided randomized anti-obesity feasibility study with adolescent Latino females. Complement Ther Med. 2016;28:22–8. https://doi.org/10.1016/j.ctim.2016.07.006. (Epub 2016 Aug 1. PMID: 27670866.
Kulendran M, King D, Schmidtke KA, Curtis C, Gately P, Darzi A, Vlaev I. The use of commitment techniques to support weight loss maintenance in obese adolescents. Psychol Health. 2016;31(11):1332–41. https://doi.org/10.1080/08870446.2016.1204452. Epub 2016 Aug 12. PMID: 27406781.
Pbert L, Druker S, Barton B, Schneider KL, Olendzki B, Gapinski MA, Kurtz S, Osganian S. A school-based program for overweight and obese adolescents: a randomized controlled trial. J Sch Health. 2016;86(10):699–708. https://doi.org/10.1111/josh.12428. PMID: 27619760; PMCID: PMC5033122.
Larsen LM, Hertel NT, Mølgaard C, Christensen RD, Husby S, Jarbøl DE. Early intervention for childhood overweight: a randomized trial in general practice. Scand J Prim Health Care. 2015;33(3):184–90. https://doi.org/10.3109/02813432.2015.1067511. Epub 2015 Jul 20. PMID: 26194172; PMCID: PMC4750722.
Kulik N, Ennett ST, Ward DS, Bowling JM, Fisher EB, Tate DF. Brief report: a randomized controlled trial examining peer support and behavioral weight loss treatment. J Adolesc. 2015;44:117–23. https://doi.org/10.1016/j.adolescence.2015.07.010. Epub 2015 Aug 7. PMID: 26265590.
Norman G, Huang J, Davila EP, Kolodziejczyk JK, Carlson J, Covin JR, Gootschalk M, Patrick K. Outcomes of a 1-year randomized controlled trial to evaluate a behavioral “stepped-down” weight loss intervention for adolescent patients with obesity. Pediatr Obes. 2016;11(1):18–25. https://doi.org/10.1111/ijpo.12013. Epub 2015 Feb 19. PMID: 25702630; PMCID: PMC4544661.
Parra-Medina D, Mojica C, Liang Y, Ouyang Y, Ramos AI, Gomez I. Promoting weight maintenance among overweight and obese Hispanic children in a rural practice. Child Obes. 2015;11(4):355–63. https://doi.org/10.1089/chi.2014.0120. Epub 2015 May 7. PMID: 25950140; PMCID: PMC4529103.
Serra-Paya N, Ensenyat A, Castro-Viñuales I, Real J, Sinfreu-Bergués X, Zapata A, Mur JM, Galindo-Ortego G, Solé-Mir E, Teixido C. Effectiveness of a multi-component intervention for overweight and obese children (Nereu Program): a randomized controlled trial. PLoS One. 2015;10(12):e0144502. https://doi.org/10.1371/journal.pone.0144502. PMID: 26658988; PMCID: PMC4684233.
Taveras EM, Marshall R, Kleinman KP, Gillman MW, Hacker K, Horan CM, Smith RL, Price S, Sharifi M, Rifas-Shiman SL, Simon SR. Comparative effectiveness of childhood obesity interventions in pediatric primary care: a cluster-randomized clinical trial. JAMA Pediatr. 2015;169(6):535–42. https://doi.org/10.1001/jamapediatrics.2015.0182. PMID: 25895016.
Steele RG, Jensen CD, Gayes LA, Leibold HC. Medium is the message: Moderate parental control of feeding correlates with improved weight outcome in a pediatric obesity intervention. J Pediatr Psychol. 2014;39(7):708–17. https://doi.org/10.1093/jpepsy/jsu035.
van der Baan-Slootweg O, Benninga MA, Beelen A, van der Palen J, Tamminga-Smeulders C, Tijssen JG, van Aalderen WM. Inpatient treatment of children and adolescents with severe obesity in the Netherlands: a randomized clinical trial. JAMA Pediatr. 2014;168(9):807–14. https://doi.org/10.1001/jamapediatrics.2014.521. PMID: 25022831.
Wright K, Suro Z. Using community–academic partnerships and a comprehensive school-based program to decrease health disparities in activity in school-aged children. J Prev Interv Community. 2014;42(2):125–39. https://doi.org/10.1080/10852352.2014.881185. PMID: 24702663.
Danielsen YS, Nordhus IH, Júlíusson PB, Mæhle M, Pallesen S. Effect of a family-based cognitive behavioural intervention on body mass index, self-esteem and symptoms of depression in children with obesity (aged 7–13): a randomised waiting list controlled trial. Obes Res Clin Pract. 2013;7(2):e116–28. https://doi.org/10.1016/j.orcp.2012.06.003. PMID: 24331773.
Davis AM, Sampilo M, Gallagher KS, Landrum Y, Malone B. Treating rural pediatric obesity through telemedicine: outcomes from a small randomized controlled trial. J Pediatr Psychol. 2013;38(9):932–43. https://doi.org/10.1093/jpepsy/jst005. Epub 2013 Feb 21. PMID: 23428652; PMCID: PMC3785218.
Johnston CA, Moreno JP, Gallagher MR, Wang J, Papaioannou MA, Tyler C, Foreyt JP. Achieving long-term weight maintenance in Mexican-American adolescents with a school-based intervention. J Adolesc Health. 2013;53(3):335–41.
Lochrie AS, Wysocki T, Hossain J, Milkes A, Antal H, Buckloh L, Canas JA, Bobo E, Lang J. The effects of a family-based intervention (FBI) for overweight/obese children on health and psychological functioning. Clin Pract Pediatr Psychol. 2013;1(2):159–70.
O’Connor TM, Hilmers A, Watson K, Baranowski T, Giardino AP. Feasibility of an obesity intervention for paediatric primary care targeting parenting and children: Helping HAND. Child Care Health Dev. 2013;39(1):141–9. https://doi.org/10.1111/j.1365-2214.2011.01344.x. Epub 2011 Nov 9. PMID: 22066521.
Saelens BE, Lozano P, Scholz K. A randomized clinical trial comparing delivery of behavioral pediatric obesity treatment using standard and enhanced motivational approaches. J Pediatr Psychol. 2013;38(9):954–64. https://doi.org/10.1093/jpepsy/jst054. Epub 2013 Jul 31. PMID: 23902797; PMCID: PMC3785221.
Verbeken S, Braet C, Goossens L, van der Oord S. Executive function training with game elements for obese children: a novel treatment to enhance self-regulatory abilities for weight-control. Behav Res Ther. 2013;51(6):290–9. https://doi.org/10.1016/j.brat.2013.02.006. Epub 2013 Mar 4. PMID: 23524063.
Wright JA, Phillips BD, Watson BL, Newby PK, Norman GJ, Adams WG. Randomized trial of a family-based, automated, conversational obesity treatment program for underserved populations. Obesity (Silver Spring). 2013;21(9):E369–78. https://doi.org/10.1002/oby.20388. Epub 2013 Jun 11. PMID: 23512915; PMCID: PMC3695059.
Nemet D, Ben-Haim I, Pantanowits M, Eliakim A. Effects of a combined intervention for treating severely obese prepubertal children. J Pediatr Endocrinol Metab. 2013;26(1–2):91–6. https://doi.org/10.1515/jpem-2012-0225. PMID: 23382300.
Croker H, Viner RM, Nicholls D, Haroun D, Chadwick P, Edwards C, Wells JC, Wardle J. Family-based behavioural treatment of childhood obesity in a UK National Health Service setting: randomized controlled trial. Int J Obes (Lond). 2012;36(1):16–26. https://doi.org/10.1038/ijo.2011.182. Epub 2011 Sep 20. PMID: 21931327; PMCID: PMC3272466.
Fullerton G, Tyler C, Johnston CA, Vincent JP, Harris GE, Foreyt JP. Quality of life in Mexican-American children following a weight management program. Obesity (Silver Spring). 2007;15(11):2553–6. https://doi.org/10.1038/oby.2007.306. PMID: 18070745.
Lloyd-Richardson EE, Jelalian E, Sato AF, Hart CN, Mehlenbeck R, Wing RR. Two-year follow-up of an adolescent behavioral weight control intervention. Pediatrics. 2012;130(2):e281–8. https://doi.org/10.1542/peds.2011-3283. Epub 2012 Jul 2. PMID: 22753560; PMCID: PMC3408687.
Nguyen B, Shrewsbury VA, O’Connor J, Steinbeck KS, Lee A, Hill AJ, Shah S, Kohn MR, Torvaldsen S, Baur LA. Twelve-month outcomes of the loozit randomized controlled trial: a community-based healthy lifestyle program for overweight and obese adolescents. Arch Pediatr Adolesc Med. 2012;166(2):170–7. https://doi.org/10.1001/archpediatrics.2011.841. PMID: 22312175.
Toulabi T, KhoshNiyatNikoo M, Amini F, Nazari H, Mardani M. The influence of a behavior modification interventional program on body mass index in obese adolescents. J Formos Med Assoc. 2012;111(3):153–9. https://doi.org/10.1016/j.jfma.2011.05.007. Epub 2012 Mar 3. PMID: 22423669.
Vos RC, Huisman SD, Houdijk EC, Pijl H, Wit JM. The effect of family-based multidisciplinary cognitive behavioral treatment on health-related quality of life in childhood obesity. Qual Life Res. 2012;21(9):1587–94. https://doi.org/10.1007/s11136-011-0079-1. Epub 2011 Dec 8. PMID: 22161746.
Díaz RG, Esparza-Romero J, Moya-Camarena SY, Robles-Sardín AE, Valencia ME. Lifestyle intervention in primary care settings improves obesity parameters among Mexican youth. J Am Diet Assoc. 2010;110(2):285–90. https://doi.org/10.1016/j.jada.2009.10.042. PMID: 20102858.
Kalarchian MA, Levine MD, Arslanian SA, Ewing LJ, Houck PR, Cheng Y, Ringham RM, Sheets CA, Marcus MD. Family-based treatment of severe pediatric obesity: randomized, controlled trial. Pediatrics. 2009;124(4):1060–8. https://doi.org/10.1542/peds.2008-3727. Epub 2009 Sep 28. PMID: 19786444; PMCID: PMC2935494.
Kitzman-Ulrich H, Hampson R, Wilson DK, Presnel K, Brown A, O’Boyle M. An adolescent weight-loss program integrating family variables reduces energy intake. J Am Diet Assoc. 2009;109(3):491–6. https://doi.org/10.1016/j.jada.2008.11.029. PMID: 19248868.
Sabet Sarvestani R, Jamalfard MH, Kargar M, Kaveh MH, Tabatabaee HR. Effect of dietary behaviour modification on anthropometric indices and eating behaviour in obese adolescent girls. J Adv Nurs. 2009;65(8):1670–5. https://doi.org/10.1111/j.1365-2648.2009.05029.x. Epub 2009 Jun 1. PMID: 19493149.
Hughes AR, Stewart L, Chapple J, McColl JH, Donaldson MD, Kelnar CJ, Zabihollah M, Ahmed F, Reilly JJ. Randomized, controlled trial of a best-practice individualized behavioral program for treatment of childhood overweight: Scottish Childhood Overweight Treatment Trial (SCOTT). Pediatrics. 2008;121(3):e539–46. https://doi.org/10.1542/peds.2007-1786. PMID: 18310175.
Munsch S, Roth B, Michael T, Meyer AH, Biedert E, Roth S, Speck V, Zumsteg U, Isler E, Margraf J. Randomized controlled comparison of two cognitive behavioral therapies for obese children: mother versus mother-child cognitive behavioral therapy. Psychother Psychosom. 2008;77(4):235–46. https://doi.org/10.1159/000129659. Epub 2008 Apr 28. PMID: 18443390.
Savoye M, Shaw M, Dziura J, Tamborlane WV, Rose P, Guandalini C, Goldberg-Gell R, Burgert TS, Cali AM, Weiss R, Caprio S. Effects of a weight management program on body composition and metabolic parameters in overweight children: a randomized controlled trial. JAMA. 2007;297(24):2697–704. https://doi.org/10.1001/jama.297.24.2697. PMID: 17595270.
Williamson DA, Walden HM, White MA, York-Crowe E, Newton RL Jr, Alfonso A, Gordon S, Ryan D. Two-year internet-based randomized controlled trial for weight loss in African-American girls. Obesity (Silver Spring). 2006;14(7):1231–43. https://doi.org/10.1038/oby.2006.140. PMID: 16899804.
Jiang JX, Xia XL, Greiner T, Lian GL, Rosenqvist U. A two year family based behaviour treatment for obese children. Arch Dis Child. 2005;90(12):1235–8. https://doi.org/10.1136/adc.2005.071753. Epub 2005 Sep 27. PMID: 16188958; PMCID: PMC1720215.
Herrera EA, Johnston CA, Steele RG. A comparison of cognitive and behavioral treatments for pediatric obesity. Child Health Care. 2004;33(2):151–67.
Goldfield GS, Epstein LH, Kilanowski CK, Paluch RA, Kogut-Bossler B. Cost-effectiveness of group and mixed family-based treatment for childhood obesity. Int J Obes Relat Metab Disord. 2001;25(12):1843–9. https://doi.org/10.1038/sj.ijo.0801838. PMID: 11781766.
Epstein LH, McKenzie SJ, Valoski A, Klein KR, Wing RR. Effects of mastery criteria and contingent reinforcement for family-based child weight control. Addict Behav. 1994;19(2):135–45. https://doi.org/10.1016/0306-4603(94)90038-8.
Davoli AM, Broccoli S, Bonvicini L, Fabbri A, Ferrari E, D’Angelo S, et al. Pediatrician-led motivational interviewing to treat overweight children: an RCT. Pediatrics. 2013;132(5):e1236–46.
Grønbaek H, Madsen S, Michaelsen K. Family involvement in the treatment of childhood obesity: the Copenhagen approach. Eur J Pediatr. 2009;168(12):1437–47.
Small L, Bonds-McClain D, Melnyk B, Vaughan L, Gannon AM. The preliminary effects of a primary care–based randomized treatment trial with overweight and obese young children and their parents. J Pediatr Health Care. 2014;28(3):198–207.
Taveras EM, Gortmaker SL, Hohman KH, Horan CM, Kleinman KP, Mitchell K, et al. Randomized controlled trial to improve primary care to prevent and manage childhood obesity: the high five for kids study. Arch Pediatr Adolesc Med. 2011;165(8):714–22.
Van den Akker EL, Puiman PJ, Groen M, Timman R, Jongejan MT, Trijsburg W. A cognitive behavioral therapy program for overweight children. J Pediatr. 2007;151(3):280–3.
van Grieken A, Veldhuis L, Renders CM, Borsboom GJ, van der Wouden JC, Hirasing RA, et al. Population-based childhood overweight prevention: outcomes of the ‘Be active, eat right’study. PLoS ONE. 2013;8(5): e65376.
Watson PM, Dugdill L, Pickering K, Owen S, Hargreaves J, Staniford LJ, et al. Service evaluation of the GOALS family-based childhood obesity treatment intervention during the first 3 years of implementation. BMJ Open. 2015;5(2): e006519.
Wong EM, Cheng MM. Effects of motivational interviewing to promote weight loss in obese children. J Clin Nurs. 2013;22(17–18):2519–30.
Schwartz RP, Hamre R, Dietz WH, Wasserman RC, Slora EJ, Myers EF, et al. Office-based motivational interviewing to prevent childhood obesity: a feasibility study. Arch Pediatr Adolesc Med. 2007;161(5):495–501.
Nobles J, Radley D, Dimitri P, Sharman K. Psychosocial interventions in the treatment of severe adolescent obesity: The SHINE program. J Adolesc Health. 2016;59(5):523–9.
Sacher PM, Kolotourou M, Chadwick PM, Cole TJ, Lawson MS, Lucas A, et al. Randomized controlled trial of the MEND program: a family-based community intervention for childhood obesity. Obesity. 2010;18(S1):S62–8.
Baños RM, Cebolla A, Botella C, García-Palacios A, Oliver E, Zaragoza I, et al. Improving childhood obesity treatment using new technologies: the ETIOBE system. Clin Pract Epidemiol Mental Health: CP & EMH. 2011;7:62.
Moraes AS, Padovani RC, La Scala Teixeira CV, Cuesta MGS, Gil SDS, de Paula B, dos Santos GM, Gonçalves RT, Dâmaso AR, Oyama LM, Gomes RJ, Caranti DA. Cognitive behavioral approach to treat obesity: a randomized clinical trial. Front Nutr. 2021;8:611217. https://doi.org/10.3389/fnut.2021.611217.
Hyde H, McPeters SL. Motivational interviewing screening tool to address pediatric obesity. J Nurse Pract. 2022;18(3):289–93.
Borrello M, Pietrabissa G, Ceccarini M, Manzoni GM, Castelnuovo G. Motivational Interviewing in childhood obesity treatment. Front Psychol. 2015;6:1732. https://doi.org/10.3389/fpsyg.2015.01732.
Boisvert JA, Harrell WA. Integrative treatment of pediatric obesity: psychological and spiritual considerations. Integr Med (Encinitas). 2015;14(1):40–7 PMID: 26770130; PMCID: PMC4566459.
Pamungkas RA, Chamroonsawasdi K. Home-based interventions to treat and prevent childhood obesity: a systematic review and meta-analysis. Behav Sci (Basel). 2019;9(4):38. https://doi.org/10.3390/bs9040038. PMID: 31013841; PMCID: PMC6523065.
Peña MM, Dixon B, Taveras EM. Are you talking to ME? The importance of ethnicity and culture in childhood obesity prevention and management. Child Obes. 2012;8(1):23–7. https://doi.org/10.1089/chi.2011.0109. PMID: 22799474; PMCID: PMC3647541.
Acknowledgements
This article is dedicated to “Professor Carsten Lyng Obel”- who passed away in February 2022- in memory of his contribution to the conception of this study.
Funding
Open access funding provided by University Library of Southern Denmark This work was done without any fund.
Author information
Authors and Affiliations
Contributions
FB conceived and designed the review, participated in literature review, data extraction, quality assessment of the studies, interpretation of the results and wrote the manuscript. SHJ participated in literature review and data extraction. MQ conceived and designed the review, conducting the meta-analyses, and participated in interpretation of the results. ALS participated in quality assessment of the studies and revised the manuscript. MKA and TT revised the manuscript. JBN and BLH contributed to the conception of the study and revised the manuscript critically. All the authors approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search strategy.
Additional file 2.
Characteristics of the included studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Baygi, F., Djalalinia, S., Qorbani, M. et al. The effect of psychological interventions targeting overweight and obesity in school-aged children: a systematic review and meta-analysis. BMC Public Health 23, 1478 (2023). https://doi.org/10.1186/s12889-023-16339-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16339-7